A subpopulation of the immune cells targeted by HIV may play an important role in controlling viral loads after initial infection, potentially helping to determine how quickly infection will progress. In the February 29 issue of Science Translational Medicine, a team of researchers from the Ragon Institute of Massachusetts General Hospital (MGH), MIT and Harvard describe finding a population of HIV-specific CD4 T cells – cells traditionally thought to direct and support activities of other immune cells – that can directly kill HIV-infected cells.
“We observed the emergence of CD4 T cells able to kill HIV-infected cells in those patients who are able to control viral replication soon after acute infection,” says Hendrik Streeck, MD, PhD, a Ragon Institute faculty member and senior author of the report. “These cells appear very early in HIV infection, and we believe they may set the stage for the course of the disease.”
The primary role of CD4 T cells is to assist other cells of the immune system; and their importance is illustrated by how completely the immune response collapses after the cells, the main cellular targets of HIV, are destroyed. Ironically, CD4 cells that are specifically targeted against HIV are preferentially infected and depleted by the virus.
However, although HIV-specific CD4 cells have not been a major focus of vaccine research, these cells may have an important role in controlling HIV infection. “Every successful licensed vaccine induces CD4 T cell responses to some extent,” Streeck explains, “and we know from many other viral infections that the success of the immune system in gaining control is best achieved in the presence of strong CD4 T cell responses.”
To investigate whether CD4 T cell responses are important in the early control of HIV infection, the Ragon Institute team enrolled a group of 11 volunteers who were in the earliest stages of HIV infection, a time when viral levels are exceedingly high. A year into the study, participants were divided into two groups based on the level of HIV in their bodies – one group was able to keep HIV at low levels while the other group apparently had no immune control over HIV replication. Retrospective analysis of samples taken throughout the year showed striking differences in the CD4 T cell responses in both groups. While the HIV-specific CD4 responses in the group that did not control HIV replication quickly dropped and stayed low, the same response increased significantly in participants able to effectively control the virus, suggesting a role for HIV-specific CD4 cells in viral control.
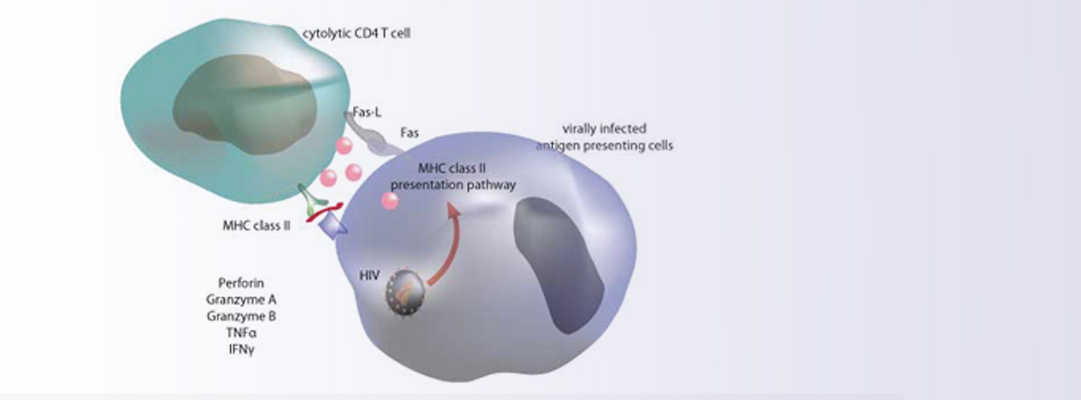
Additional experiments revealed that the HIV-specific CD4 T cell responses showed activity associated with cell-killing and could even destroy HIV-infected macrophages – an unusual function for CD4 T cells, which have traditionally been seen as helper cells. In addition, the researchers determined that the presence of a specific cell-death protein called granzyme A prominently distinguished HIV-specific CD4 cells of participants maintaining a lower “viral set point” from those less able to control viral levels.
To validate these findings, the researchers examined a larger group of HIV-infected individuals and found that those with higher levels of granzyme A in their HIV-specific CD4 T cell response immediately after infection progressed more slowly to AIDS and did not require antiretroviral therapy as quickly as did those with lower levels of the protein. “The key baseline difference between these two groups has to do with the quality, not the quantity, of the HIV-specific CD4 T cell response,” explains Streeck, an assistant professor of Medicine at Harvard Medical School. “In those who progressed to a lower viral set point, the early CD4 response was dominated by granzyme A expression, which was highly predictive of the rate of disease progression.”
Associating a particular CD4 T cell activity with more successful suppression of viral levels suggests that inducing such responses with a vaccine may be beneficial, Streeck notes. In addition, the association of granzyme A expression with a more effective HIV-specific CD4 cell response suggests that measuring levels of the protein may allow prediction of disease outcome at the earliest stages of infection, something which is not currently possible. Future studies will need to explore the mechanisms underlying the cell-killing activities of the CD4 cell response and the functional and prognostic role of granzyme A.
The lead author of the Science Translational Medicine report is Damien Soghoian of the Ragon Institute. Additional co-authors are Michael Flanders, Kailan Sierra-Davidson, Sam Butler, Thomas Pertel, PhD, Srinika Ranasinghe, PhD, Madelene Lindqvist, Isaiah Davis, Kimberly Lane, Alicja Piechocka-Trocha, Abraham Brass, MD, PhD, and Bruce Walker, MD, Ragon Institute of Mass General, MIT, and Harvard; Heiko Jessen, MD, Practice Jessen-Jesse-Stein, Berlin, Germany; Jenna Rychert, MD, and Eric Rosenberg, MD, MGH Infectious Disease Unit; and Jason Brenchley, PhD, National Institutes of Health. The study was funded by the National Institute for Allergy and Infectious Diseases of the National Institutes of Health.
The Ragon Institute of Mass General, MIT, and Harvard was established in 2009 with a gift from the Phillip T. and Susan M. Ragon Foundation, creating a collaborative scientific mission among these institutions to harness the immune system to combat and cure human diseases. The primary initial focus of the institute is to contribute to the development of an effective AIDS vaccine. Administratively based at Massachusetts General Hospital, the Ragon Institute draws scientists and engineers from diverse backgrounds and areas of expertise across the Harvard and MIT communities and throughout the world, in order to apply the full arsenal of scientific knowledge to understanding mechanisms of immune control and immune failure and to apply these advances to directly benefit patients.
Media Contacts: Sarah Dionne, 617-726-6126, [email protected]
Sue McGreevey, 617 724-2764, [email protected]