
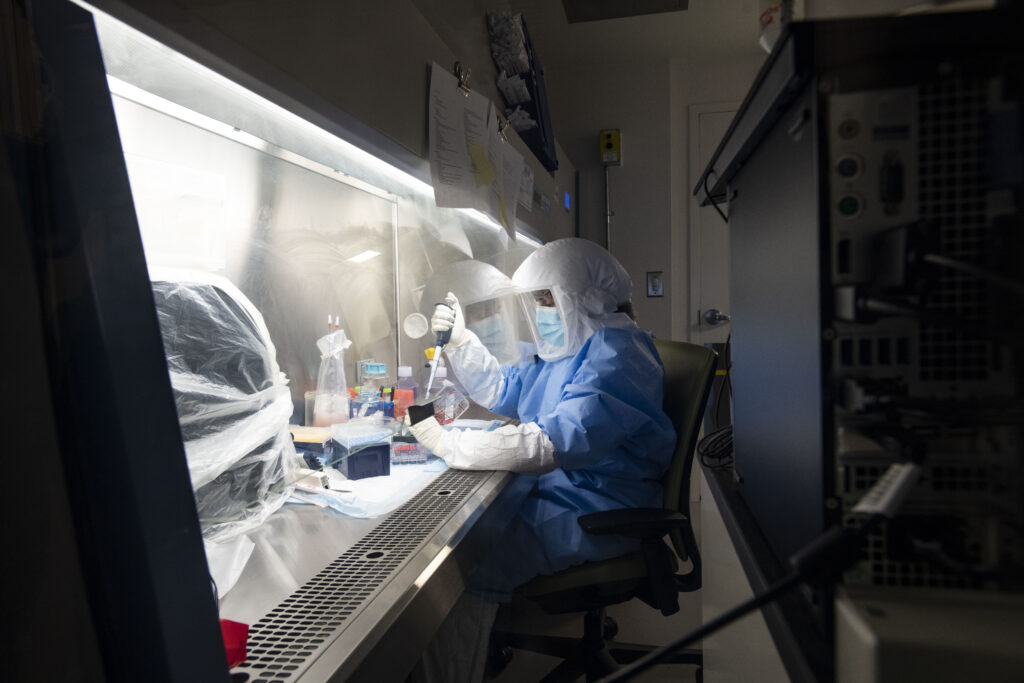
The Ragon’s Biosafety Level 3 lab plays a key role in translational studies of emerging viral infections
When scientists want to study potentially dangerous pathogens—bacteria, viruses, or other organisms that can cause disease—they need to use specialized laboratory spaces. At the Ragon Institute, our state-of-the-art Biosafety Level 3 (BSL-3) laboratory is where experiments can be performed on pathogens that have the potential to cause serious or even fatal infections. This resource has been important for the study of emerging infectious disease outbreaks such as SARS-CoV-2 and monkeypox over the past two years, and it allows scientists from all over the Greater Boston area and beyond to work together on indispensable research.
The Ragon’s BSL-3 lab is one of only eight in Massachusetts and about 200 throughout the U.S. BSL-3 labs have rigorous requirements for design, airflow and exhaust that allow work on certain infectious diseases to be performed in a safe manner. Before an employee can enter the BSL-3 lab, they must undergo specialized training—and don head-to-toe personal protective equipment including gowns and hoods with face shields. Access to the lab is tightly controlled. (A higher level not found at the Ragon, BSL-4, is for work with extremely dangerous and deadly infectious agents, such as Ebola. There are currently only about 60 BSL-4 labs worldwide.) In 2020, the BSL-3 lab underwent upgrades that expanded its capabilities for virology research through a generous gift from Mark and Lisa Schwartz, allowing the BSL-3 to safely be used to research SARS-CoV-2 and make a worldwide impact on understanding infectious disease. It’s become a crucial resource for collaborators working together to study the virus.
“By CDC requirement, there are precautions that need to be taken when handling SARS-CoV-2 samples. So while you can process blood samples and things like that in BSL-2-plus, actually trying to grow virus needs to be done in a BSL-3 lab,” says Julie Boucau, PhD, senior research scientist at the Ragon and co-director of the BSL-3 with Yong (Mike) Xie, PhD. “There are few places around the Boston area that can do it … so people work by collaboration with BSL-3 labs,” she says.
Boucau is the first author on three recent papers published in June that involved BSL-3 work in collaboration with colleagues at multiple institutions. All three studies looked at data collected during the ongoing cohort study POSt-VaccInaTIon Viral CharactEristics Study (POSITIVES), in which researchers obtain nasal swabs from individuals infected with SARS-CoV-2 to characterize new variants, how long COVID-19 is contagious, how the immune system responds to infection, and the efficacy of treatment.
POSITIVES is led by four principal investigators: Ragon member Amy Barczak, MD, scientific director of the Ragon’s BSL-3 who recently became the Director of Research of the MGH Infectious Diseases DivisionMassachusetts Consortium on Pathogen Readiness (MassCPR), a collaboration convened by Harvard Medical School and co-led by Ragon Institute Founding Director Bruce Walker.

These four researchers specialize in different areas and had largely not worked together before COVID. Barczak’s lab has historically focused on tuberculosis, Li’s lab has studied HIV, Lemieux has researched tick-borne diseases such as Lyme disease, and Siedner is a clinical epidemiologist who has conducted HIV research in southwestern Uganda.
“I think this is probably the best example I’ve been involved in that really shows the power of organic science and the ability to transition questions from the hospital from the clinic to the lab to find answers to some of the most important public health questions,” Siedner says. “This collaboration started with a group of early-career scientists who were all working in the midst of the COVID-19 epidemic as clinical infectious disease doctors realizing that there are some really important questions that we just didn’t have the answers to.”
One study that came out of this collaboration, published in the New England Journal of Medicine, looked at the duration of shedding of SARS-CoV-2 in viral culture, that is, how long nasal swabs from infected individuals could be used to grow live SARS-CoV-2 in the lab. The researchers wondered if people infected with Omicron, which had been shown to be less severe, especially in vaccinated individuals, would shed the virus for a shorter period of time. “We learned that wasn’t the case,” Siedner says. They found that people with Omicron tend to shed live virus for on average around six to eight days; at least 25 percent of people in the study shed the virus for ten days or more. These findings suggest that the CDC’s current guideline to quarantine for five says, which was shortened from ten days last December, may not be enough to prevent transmission in all cases. “I think people should be aware that irrespective of what guidelines say, there is a reasonable chance that if you get infected by Omicron, you still are shedding virus that’s alive and potentially transmissible [after five days],” he says.
Culturing the virus in the lab is a surrogate marker; being able to grow live virus from a patient’s nasal swab doesn’t directly prove that they are contagious. But it’s the best tool scientists have right now for making an educated guess. “The real problem, I think, from a practicality standpoint, is how do you prove contagiousness … certainly it wouldn’t be safe or ethical to have people interacting with others and then potentially transmitting the virus to other people,” Siedner says. Looking at culturable virus as a proxy for infectiousness is “probably the safest thing you can do ethically, short of actually watching people transmit the virus to others,” he says.
Another study using POSITIVES data, published in Cell Reports Medicine, examined patients treated with the monoclonal antibody (mAb) bamlanivimab. Historically, monoclonal antibodies have been an effective means of COVID-19 treatment, and the researchers wanted to look at the ability of monoclonal antibodies to affect viral culture. According to Li, the researchers wanted to answer the question, “Are there ways to look at the impact of monoclonal antibodies more rapidly than just waiting for someone to be hospitalized?”
The results were “striking,” he says. They found that zero out of 28 patients treated with bamlanivimab still had culturable SARS-CoV-2 virus one day after treatment. “Viral culture, I think, could really be used as a surrogate marker for monoclonal antibody efficacy, and this could potentially lead to a way to complete trials much more rapidly than just waiting for long-term clinical efficacy,” he says.
Additionally, there are implications for public health. “It appears that individuals who are treated with monoclonal antibodies, in addition to being protected from severe disease, may be less likely to transmit virus to those around them,” Li says.
A third study, published in Clinical Infectious Diseases, looked at virologic rebound in several patients after treatment with nirmatrelvir-ritonavir, commonly known as Paxlovid. The study arose following reports that some people treated with Paxovid have experienced rebound COVID-19 symptoms. “What we found was that this is real, that people are relapsing, that the virus does come back, and that it comes back almost exactly the same as the initial infection, so it’s almost impossible to tell the difference between the two,” Siedner says. “We did find that people who relapse had virus that we could grow in culture, meaning that it’s potentially contagious, and so their isolation, which was typically ending between five and ten days, really needs to be restarted,” he says.
The researchers are recruiting for a larger study now to try to get a better estimate of how often this occurs. Still, Paxlovid is extremely effective at preventing severe COVID-19 symptoms, Siedner says, pointing out that in clinical trials, patients had an 80-90 percent reduction in hospitalization or death. “Its benefits, even with rebounds, are likely to far outweigh the risk, especially in high-risk people,” he says.
With today’s increased global connectivity, it is easier than ever for infectious diseases to spread, as the world has seen with COVID and now with the spread of monkeypox. The World Health Organization declared monkeypox a global health emergency on July 23, and multiple U.S. states have also declared states of emergency. “Anything that happens in one place in the world impacts the entire world, and that is only predicted to increase over the following decades,” Barczak says. Researchers who use the BSL-3 are positioned to quickly and effectively pivot to studying emerging infectious disease situations, and research on monkeypox in the BSL-3 is currently underway.
“We are uniquely positioned to address current and future outbreaks,” Barczak says, adding that the Ragon’s BSL-3 resources are aimed at making this type of research accessible to institutions that don’t have their own BSL-3 lab. “It opens up the capability of the entire Boston research community.”
Are you a researcher from an academic institution who would like to make use of the Ragon’s BSL-3? Your lab members can come to our BSL-3 for training to do experiments here, or our BSL-3 team can carry out the experiments themselves and charge a fee. Please contact [email protected] for more information.
